Early in my career as a child and adolescent psychiatrist, I encountered a case that has stayed with me in the many years since. A 15-year-old girl was referred to me with severe depression and suicidal thoughts. She had recently discovered that she was pregnant. Her parents were devastated and had threatened to disown her. The girl felt ashamed, frightened and utterly alone. She also refused antidepressant medication. Everyone involved in her care felt stuck. Her doctors were worried about her safety; her parents were angry and heartbroken; and the young girl herself had lost hope that things could improve. I asked to meet the girl and later her parents. The conversations were difficult, with tears, anger and long silences. But slowly, something started to shift. The parents began to hear their daughter’s fears. The daughter began to understand the depth of her parents’ disappointment and pain. Eventually, her mother agreed to support her during the pregnancy and help care for the baby after birth. In the end, she recovered without needing medication. The moment that remains most vivid to me came when her father finally told her that, despite everything that had happened, “I still love you”.
In situations like these, doctors are sometimes tempted to focus on the clinical problem in front of them. But adolescent care is rarely just about symptoms and treatment plans. It is about relationships. For that family, healing did not come from a prescription. It came from rebuilding trust.
Cases like this illustrate the complexity of caring for young people. Adolescents often come to doctors with concerns that they do not want their parents to know about. These may involve mental health struggles, sexual health issues, substance use or deeply personal questions about identity. When this happens, doctors face a difficult question: how much autonomy should a young person have in decisions about their own health?
Extent of a young person's autonomy
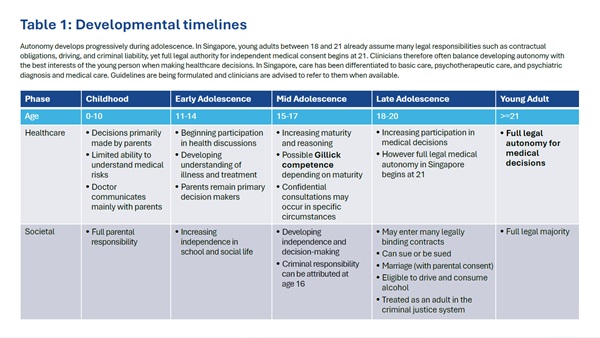
The concept of Gillick competence offers some guidance. Originating from a landmark British case in 1986, it recognises that adolescents may have sufficient maturity and understanding to participate meaningfully in decisions about their care, even though they are not yet legal adults. In Singapore, the Children and Young Person’s Act defines a child as a person under the age of 14 years, while a young person is defined as someone aged 14 years or older but below 18 years old. 21 years is the formal “age of majority” where individuals gain significant commercial and personal rights of adults (see Table 1 for further elaboration).
But Gillick competence is often misunderstood. It does not mean that teenagers can simply make medical decisions on their own, nor does it mean that parents should be excluded from care. Instead, it reminds doctors that young people themselves have voices that deserve to be heard.
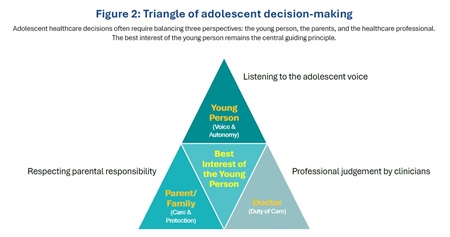
At the same time, clinicians have a duty to act in the best interests of the young person, and this remains the guiding principle in caring for minors. Balancing these responsibilities requires discerning judgement rather than rigid rules.
When confidentiality is requested
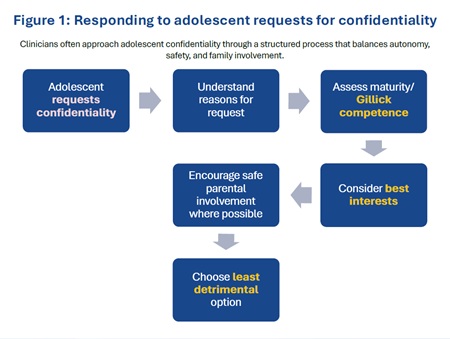
One of the most challenging situations arises when an adolescent asks a doctor to keep information confidential from their parents. A teenage girl may request emergency contraception but insist that her parents must not be informed. Another young person may seek treatment for a sexually transmitted infection while fearing severe punishment in the event the family finds out about it. A depressed teenager may ask for counselling while refusing parental involvement. If doctors insist on parental consent in every situation, many adolescents will simply avoid seeking help altogether. Worse, they may seek help through illegal means, and that outcome serves no one. Yet automatically granting confidentiality without careful consideration can undermine the family relationships that often support recovery. The most important question therefore becomes: why does this young person want confidentiality?
Understanding the reasons behind the request often reveals more than the request itself. Sometimes, the fear is rooted in embarrassment or misunderstanding. Other times, it reflects genuine family conflict or cultural stigma. There is another ethical principle that is especially useful in these situations: “the least detrimental alternative”. Described in the book Beyond the Best Interests of the Child by Joseph Goldstein, Anna Freud and Albert Solnit, this principle was proposed as a more realistic and urgent replacement for the “best interests of the child” standard. Sometimes, every option carries risk. Informing parents may damage trust and discourage the adolescent from seeking future help. Maintaining confidentiality may limit family support that could be beneficial. The role of the doctor is not simply to apply rules but to choose the course of action that is least likely to harm the young person overall. Often this means trying to bring parents into the conversation gradually rather than abruptly breaching confidentiality. Doctors frequently work with adolescents to find ways of sharing information safely with family members. The goal is rarely to exclude parents permanently. Instead, it is to preserve trust long enough for a healthier dialogue to emerge.
Complex decisions in modern adolescent care
Adolescent healthcare today presents a growing range of complex decisions. One example is gender dysphoria and gender-affirming treatment, which has attracted significant attention worldwide. These decisions can involve psychological assessment, social transition and medical interventions. Such issues require careful multidisciplinary evaluation and, wherever possible, the involvement of families.
Another dilemma arises in the treatment of depression in adolescents. Psychotherapy is recommended as the first-line treatment. Yet occasionally an adolescent may request antidepressant medication while asking that their parents not be informed. Should medication be prescribed without parental knowledge? Would psychotherapy alone be acceptable in such circumstances?
Emerging therapies create additional questions. New evidence-based approaches such as non-invasive brain stimulation and nutritional supplementation are increasingly explored in youth mental health.
Each intervention carries its own level of risk and uncertainty. Decisions about consent therefore depend not only on the maturity of the adolescent but also on the nature of the treatment.
Learning to make decisions
It is also worth remembering that decision-making is part of development. Young people make choices every day as they navigate friendships, school and social life. Some of those decisions will inevitably be bad ones. Parents and teachers recognise that learning from mistakes is part of their development, and overprotection can sometimes prevent young people from gaining the experience they need to mature.
Healthcare decisions however often carry more serious consequences. Doctors therefore have a responsibility to guide adolescents through these decisions while ensuring their safety. In many cases, the best approach is neither to grant complete independence nor to insist on parental control. Instead, the aim is to create a space where adolescents can speak openly while gradually involving the people who care for them most.
Conclusion
I often think back to the young girl I met early in my career. If her doctors had simply insisted on we might have missed the deeper crisis unfolding within her confidentiality had been handled poorly, the fragile trust needed to bring her parents into the conversation might never have developed. What ultimately helped her recover was not a legal concept or a treatment protocol, but a willingness to listen, to understand and to create space for reconciliation. When her father finally told his daughter that he still loved her despite everything that had happened, it changed the course of that family’s story.
In adolescent medicine, we often talk about autonomy, competence and consent. But sometimes the most powerful intervention is simply helping families rediscover the bonds that were there all along.