How geriatrics started
In 1984, the Ministry of Health's (MOH) Report of the Committee on the Problems of the Aged highlighted the issues of an ageing population in Singapore. Dr FJ Jayaratnam, then Head of Medical Unit I, Tan Tock Seng Hospital (TTSH), was tasked with setting up geriatric services. He visited geriatric services in the UK and linked up with the British Geriatrics Society to have local trainees sent to UK for specialist training. Since 1988, internal medicine trainees were sent to geriatric medicine departments in Glasgow, Edinburgh, Cardiff, Newcastle, Southampton, London, and subsequently to Australia, the US and Hong Kong for training. Geriatric medicine departments were set up in TTSH (1987), Alexandra Hospital (AH; 1994) and New Changi Hospital (NCH; 1998; later renamed Changi General Hospital [CGH]).
Care for the community
MOH recognised the need to go beyond hospitals and set up community services for the elderly. Thus, the Home Nursing Foundation, which had been providing community nursing since 1976, started setting up Senior Citizens' Health Care Centres (SCHCCs) to provide day rehabilitation for the elderly with mobility problems. Most of these were located in polyclinics distributed all over Singapore, with the exceptions of Kampong Ubi SCHCC and Ang Mo Kio SCHCC, which were located at a void deck and in Ang Mo Kio Community Hospital, respectively. The Department of Health Service for the Elderly (HSE) provided oversight of these SCHCCs then. Minibuses and ambulances retrofitted with spaces for wheelchairs ferried elderly to these centres for rehabilitation. Wheelchair-bound elderly living in HDB flats that were not on floors with lift landings were ferried down staircases with the help of motorised devices with caterpillar tracks ("stair crawls"). In 1994, AH also started a Geriatric Day Hospital, catering to those who had unresolved medical problems in addition to their rehabilitation needs. This was part of the larger Alexandra Geriatric Centre that comprised geriatric medicine clinics, day rehabilitation, and an Independent Living Centre displaying and selling mobility aids and other appliances. The SCHCCs also started continence clinics for the assessment and management of elderly with urinary incontinence in the community. These were run by nurses trained in continence care and supported by geriatricians.
As acute care hospitals had limited capacity for rehabilitation, community hospitals were built to provide inpatient rehabilitation beds. These were mostly run by voluntary welfare organisations (VWOs) supported through government funding. MOH also built and ran Ang Mo Kio Community Hospital for a period of time before handing over to a VWO group.
Additionally, MOH also saw the need to redevelop nursing homes. In the old days, "nursing homes" were largely old folks' homes set up by charitable organisations to look after the elderly who had no families caring for them. Volunteer doctors provided medical care while most homes did not have much nursing expertise. Residents who turned ill were promptly sent to hospitals. MOH saw the need to increase funding and improve nursing capabilities in these homes. A Resident Assessment Form (RAF), modelled after the Australian Resident Classification Index, was created to allow documentation of functional capabilities of the residents (ie, whether they needed assistance with feeding, dressing, bathing, walking and supervision of medications). The RAF could then be used to classify residents by care needs (scores were based on time-motion studies of how much nursing time was required) and funding norms were adjusted so that those with higher care needs were allocated higher funding. MOH also set requirements for nursing norms for various categories. There remained a group requiring heavy nursing care, such as patients with tracheostomies, and thus a Chronic Sick Unit was set up in the grounds of the old Woodbridge Hospital. This was eventually handed over to a VWO as well.
The late 1980s and early 1990s also saw the development of hospice care. St Joseph's Home had set up hospice beds, and a voluntary group started home care services initially under Singapore Cancer Society, which subsequently grew into the larger HCA Hospice Care. More hospice beds were added with the setting up of the Assisi Home and Hospice (currently Assisi Hospice) and Dover Park Hospice.
The concept of home care also extended to geriatrics and Tsao Foundation started the Hua Mei Mobile Clinic, a home care service providing support to the elderly in their own homes. Other home care services also evolved, including TOUCH Home Care and Care for the Elderly Foundation (Singapore)'s CODE 4 Home Care programmes.
Progress in the healthcare landscape
By the mid-1990s, there were geriatric medicine departments; community hospitals; SCHCCs that provide day rehabilitation, home medical and home nursing; nursing homes; hospices; and a chronic sick unit. HSE by then had evolved into the Department of Continuing Care in MOH. Attention was paid to funding support and elevating standards of care. In conjunction with service development, MOH continued with the training of geriatricians and gerontology-trained nurses, and set up polytechnic programmes to train physiotherapists and occupational therapists. Diploma courses were the priority then, so that more therapists could be trained in a shorter time to meet rehabilitation needs.
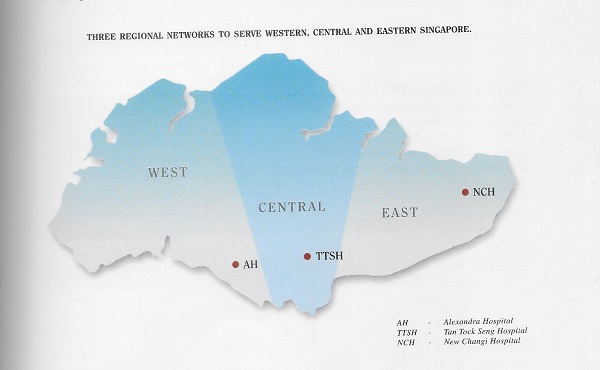
As more organisations flourished, coordination of services became more difficult. MOH decided to divide Singapore into three zones and set up three Coordinating Committees for Geriatric Care (CCGC). Thus, CCGC-West, CCGC-Central and CCGC-East were assigned to the three geographical zones. Geriatric care in each zone was supported by a geriatric medicine department with AH in the West, TTSH in the Central and NCH in the East (picture above). Around that time, the Ministry of Community Development, Youth and Sports had also set up three community care networks to coordinate social services. Many of the VWOs involved in both health and social services found themselves caught up with meetings on both sides. An Inter-Ministerial Committee (IMC) was formed and the IMC Report on The Ageing Population was published in 1999, highlighting the challenges faced by the ageing population and made recommendations across ministries.
In 2000, MOH restructured healthcare services into two clusters – National Healthcare Group (NHG) and Singapore Health Services (SingHealth) – and much of the efforts then focused on improving healthcare delivery in hospitals and primary care. Community services, largely ran by VWOs, then had to work with various hospitals and healthcare institutions. This became a greater challenge when it evolved to six clusters (ie, NHG, SingHealth, National University Health System [NUHS], Eastern Health Alliance, Alexandra Health System and Jurong Health System). Agency for Integrated Care was then set up in 2009 as a national care integrator to assist clusters' work with the VWO setting in the delivery of care. In 2017, MOH announced the reorganisation into three clusters (ie, NHG, NUHS and SingHealth). From the perspective of elderly care, this reduces complexity and allows for better co-integration with community services, not unlike the earlier plans in the mid-90s.
Going forward
Geriatric care will continue to evolve. The elderly will need a spectrum of care, including the promotion of healthy ageing; early diagnosis and management of chronic disease and age-related disorders; prompt management of complex and crisis care; rehabilitation and supportive care to maintain independence in the community; advance care planning; and end-of-life care in the final stages of their journey. Services in each cluster must address these needs in a timely and cost-effective manner. Central to service provision is the engagement of the older person and his or her family, to truly allow older people to live and leave well.
