Making ethical decisions in clinical practice is about doctors selecting the "right" choices. These "right" choices go beyond the appropriate use of current scientific knowledge, clinical reasoning and contextualisation, to the particular needs of the patient. To preserve professional integrity, decision-making needs to be consistent with the goals of medicine. The primary goals of medicine include the curing of disease, relief of suffering, improvement in functional status, as well as education and counselling. Secondary goals are training of healthcare professionals, research and clinical/professional governance. Every clinical encounter has an ethical dimension and in the majority of situations where patients and doctors have shared targets that are consistent with these goals of medicine, problems do not arise.
If patients and doctors disagree about values, then the "right" choice becomes unclear. A bleeding patient who declines blood transfusion on religious grounds is an example. In other circumstances, doctors may be faced with choices that challenge their professional values. For instance, a previously well patient admitted with pneumonia and respiratory failure may adamantly refuse mechanical ventilation. Disregarding the patient's right to refuse treatment and intubating her, or acceding to the request and allowing her to demise from a curable disease, are binary options that are both unacceptable to the majority of doctors.
These bedside ethical dilemmas are rarely resolved by simply looking up the relevant section of the Singapore Medical Council Ethical Code and Ethical Guidelines. This is because it would be unusual for an ethical conundrum to involve only a single ethical principle. Instead, these situations are often complex with competing values that directly clash. The circumstances will be unique and actual cases are rarely typical. In addition, emotions may be running high and the communication that preceded the encounter may have been less than ideal. Doctors will also be challenged to try to solve these dilemmas from foundational principles such as autonomy, beneficence, non-maleficence and justice.
A useful framework
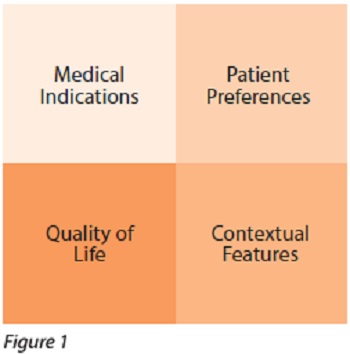
A four box tool kit was developed by Jonsen et al to assist with such ethical analysis in clinical medicine. The four boxes are headed as follows: medical indications, patient preferences, quality of life (QOL) and contextual features (see Figure 1). Just as history taking, physical examination and investigations help clarify bedside medical diagnostics, the four box ethical tool kit forms a framework to sort through the ethical elements. This framework was designed to systematically analyse and illuminate where the ethical dilemma lies. It does this by connecting the circumstances of the case to underlying ethical principles. After having identified the relevant ethical issues, the doctor can then weigh the relative contribution of each issue in analysing and resolving the dilemma. It should be noted that no single box will singlehandedly resolve the case and the order of review of the boxes do not reflect any ethical priority.
Medical indications
It is logical to start here because many ethical dilemmas arise due to unclear or even unknown goals of care. What is required is a review of the medical facts, aims of treatment, probability of treatment success and contingency in case of treatment failure. This step can also remind patients of the uncertainty that is inherent in any clinical judgement and highlight to doctors that there can be genuine disagreement in diagnosis and prognosis between equally competent clinicians.
Patient preferences
This step presumes that all healthcare providers will be truthful and respect their patient's values/choices. If the patient has intact decision-making capacity, the pertinent questions to clarify are:
- Was sufficient information provided?
- What reasonable options exist?
- Did the patient understand the information and the range of uncertainty in the clinical judgement?
- Was there any coercion in the decision-making?
In a patient without decision-making capacity, the issues that arise are:
- Was any anticipatory decision, such as the Advance Medical Directive made?
- Who has the responsibility to make decisions on the patient's behalf?
- What are the legal and ethical limits of that decision-making responsibility?
Quality of life
The improvement of QOL of those who need care can be considered a fundamental goal of medicine. Particular goals such as prevention of disease, relief of symptoms, cure of illness, prevention of an untimely death and improvement of functional status can all be related back to the QOL issue. However, a widely agreed definition of QOL remains elusive. This is because the evaluation of QOL varies with culture, age and socio-economic situation. It reflects prejudice and bias, and the notion of social worth weighs on this issue. QOL can also be used as the basis to manage resources and ultimately ration care in resource strapped healthcare systems. Healthcare providers must understand that they can have divergent interpretations of QOL from their patients and the situation can be worsened if patients are unable to express their perspectives. The guiding questions for this step are:
- Who is making the QOL evaluation?
- What are the criteria being used?
- What clinical judgements are justified based on this QOL evaluation?
Contextual features
This places the ethical dilemma in the unique context of the case and this context can create some rights and responsibilities. The cost and constraints of healthcare is an example. Beyond economic, there is also a social, legal and administrative context that has to be considered. Although this is an important step that takes into account the particular details of a given case, it is unusual for contextual features to be the decisive consideration in any ethical analysis.
Conclusion
The four box analysis does not by itself resolve any ethical conundrum. However, by anchoring facts to principles, it helps clinicians see what is ethically relevant. The dilemma is often resolved by reducing the complex case to one or two key questions. Our earlier case example of the patient with pneumonia can potentially be reframed after the four box analysis, from whether to intubate against a patient's expressed wishes, to the alternative question of whether the patient has intact decision-making capacity to decline mechanical ventilation. Getting an accurate answer to the latter question can result in far less moral distress.
The use of the four box analysis can ensure that doctors resolve ethical problems without neglecting any important issues. Just as history, physical examination and investigations are now second nature to bedside medicine, the disciplined and continued use of this framework will eventually develop the habit in doctors. Moral distress will dissipate and our patients will reap the benefits.
Further readings
- Jonsen AR, Sieglar M, Winslade WJ. Clinical Ethics: A Practical Approach to Ethical Decisions in Clinical Medicine. Sixth ed. New York: McGraw-Hill, 2010.
- Schumann JH, Alfandre D. Clinical ethical decision making: the four topics approach. Semin Med Pract 2008; 11:36-42.
- Sokol DK. The "four quadrants" approach to clinical ethics case analysis; an application and review. J Med Ethics 2008; 34:513-6.
