Part 2 – How do I choose?
This is the second part in a three-part series on how to choose a fellowship programme for specialty training. In the first article (https://bit.ly/2H0p4UZ), the importance of a fellowship and suggestions on how to start on the journey were discussed. In this instalment, we elaborate further on the factors one should consider in deciding where to go.
The journey and destination
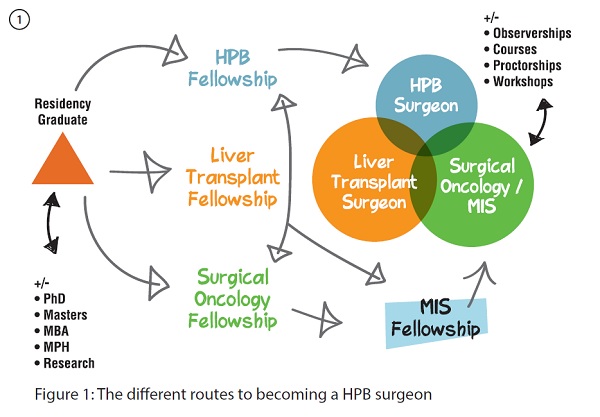
Perhaps you already have a destination in mind, but the journey there may have many routes or involve a number of detours. Choose the journey well – it is as important as the destination itself. Using hepato-pancreato-biliary (HPB) as an example, there are three traditional ways to becoming a HPB surgeon – a pure HPB fellowship, a surgical oncology fellowship (with HPB rotations) and a multi-visceral transplant fellowship (with focus on liver transplantation).1 Other non-traditional routes include a minimally invasive digestive surgery/HPB fellowship or a HPB research fellowship coupled with short observerships or proctorships. There are also what I would term as "super fellowships". These are back-to-back formal accredited fellowships, and may involve, for example, a surgical oncology fellowship followed by a HPB or a HPB/liver transplant fellowship, or a minimally invasive digestive surgery followed by a HPB fellowship or vice versa (see Figure 1). These are no doubt ideal and comprehensive but they also require commitment and hard work, notwithstanding financial constraints and time sacrifices. This is also not necessary and may be an overkill or even detrimental for some specialties. Inclan et al. reported that the additional fellowship in certain surgical fields has a significant negative impact in adjusted future earnings of the individual. For example, an additional surgical oncology or a breast fellowship adds a negative net value of over $200,000 to $300,000 to its graduates, respectively.2
The geographical location
The next question is "where?" North America currently has the most comprehensive and structured fellowship programmes with many subspecialties having their own fellowship match systems administered under various organisations (eg, The Fellowship Council and the Society of Surgical Oncology).1,3 Fellowships are also well established in many parts of Europe and Asia, albeit not administered by a central matching system.4 Most institutions outside of North America require applicants to apply to the respective programmes individually. Herein lies and illustrates another difference and potential hurdle in the application for fellowships versus basic training. Most countries have adequate basic medical education and training facilities, including residency training. However, many have not reached the maturity of developing their own structured fellowship programme.5 This leads to many graduating residents applying to established programmes abroad as international applicants. From a personal perspective, going abroad to train further comes with an array of family and social considerations, especially when undertaken at a point in life where many graduating residents are in the middle of starting or may have already started their families. As one can imagine, uprooting a young family to a foreign land for a couple of years has its own considerations. Social, financial and family issues aside, realistically, language and cultural factors cannot be over-emphasised. Being able to communicate effectively with patients and colleagues is essential to optimal functioning in a team. It is perfectly reasonable for an attending/ consultant to be able to trust and work well with the fellow before he or she allows the fellow to operate and care for his or her patients. There have been numerous examples of international fellows who felt handicapped or lost in a country where they are not able to speak fluently in the local language, however competent, well-intentioned or hardworking they were. This can result in a great deal of frustration on both ends, and the possible loss of training opportunities or a less-than-ideal educational experience. This would indeed be a tragedy, considering the investment and sacrifices that were poured into preparing for the fellowship.
The institution or the mentor
Decide on your priorities. The fellowship is a finite period, and unlike medical school and basic specialist training, it is meant to be narrow in scope and very goal-oriented. It is important to know the skill sets you want to acquire, or the disease you would like to gain more in-depth knowledge and exposure for.
For surgery and other procedural-related specialties, hands-on experience is essential. To gain experience in rare conditions or novel procedures, it is crucial to look for an institution that has the reputation or a track record of being the national (or international) referral centre, or has existing high volume and expertise. One may be able to see, manage, observe or participate in a rare procedure or condition on a weekly (or even daily) basis there, as opposed to once or twice a year elsewhere. Some institutions may have the reputation or volume, while some mentors or teams may have the skill sets or experience. Your decision should be dependent on what you aim to achieve during the fellowship stint – be it a special skill set or specific experience in managing certain conditions.
Other factors
Support from your current (and future) departmental chairs and potential hiring institutions or practices is also very important. A fellowship in an area that serves an unmet need in the current department's repertoire of services or expertise will be favourable and welcomed. This also serves to improve the spread of new knowledge and expertise to other members of the fraternity or community, leading to improved healthcare standards overall.
Real life issues are worthy of a mention here. Funding is an issue for many international applicants. Short of matched salaried positions, many fellowships worldwide do not have substantial funding aside from basic allowances for foreign fellows. Considering the costs of moving, including having to buy local malpractice insurance coverage, rental, transport and other living expenses, combined with a sudden loss of income, these can serve as the biggest barrier of entry especially when graduating residents are often bogged down with student loans and costs of starting a family, such as childcare expenses and mortgages, at this stage in their lives.2 One solution is to apply or source for funding from one's own institution or the prospective hiring practice after completion of the fellowship with a corresponding repayment system or bond in kind.
Family considerations must not be neglected. In the hectic work schedule of a fellowship, family support is important. This stint not infrequently requires moving states or across continents. One may be faced with the dilemma of leaving the family behind and slogging through the fellowship alone or uprooting the whole family, with the logistics of potential loss of spousal employment, and the change of school environments for the children; each scenario has its own slew of issues. These also include the weight given to considerations such as whether the city is a safe place to live, whether there are good schools for the kids or work available for the spouse, and so on.
This brings us to the end of the second part. In the final part of this series, we share some tips and insights on how one can try to improve their chances in obtaining that coveted fellowship position.
