In conjunction with World Breastfeeding Week, SMA organised a webinar on 1 August 2020 for our doctors on supporting new mothers in the postpartum phase. Dr Tan Yia Swam (SMA President and breast surgeon), Dr Janice Tung (gynaecologist), Sister Kang (lactation consultant) and myself (family physician) came together to share common issues faced by mothers during this phase and their management for better welfare of the mother.
The key learning points from the webinar are summarised below:
- Post-partum fever is defined as temperature more than 38 degrees Celsius on any two of the first ten days after delivery, excluding Day 1. Its risk factors include emergency caesarean delivery, prolonged labour, retained products of conception/ placenta requiring manual evacuation, preterm labour and prolonged rupture of membranes. Patients who present as such ought to be referred to a gynaecologist for in-patient management.
- Most medications prescribed to breastfeeding mothers are safe if they are:
- Commonly prescribed to infants
- Safe for use during pregnancy
- Not absorbed in the stomach/intestines
- Not excreted into the breastmilk
- Topicals applied to skin/nose
- Local, regional anaesthesia
- Immunisations
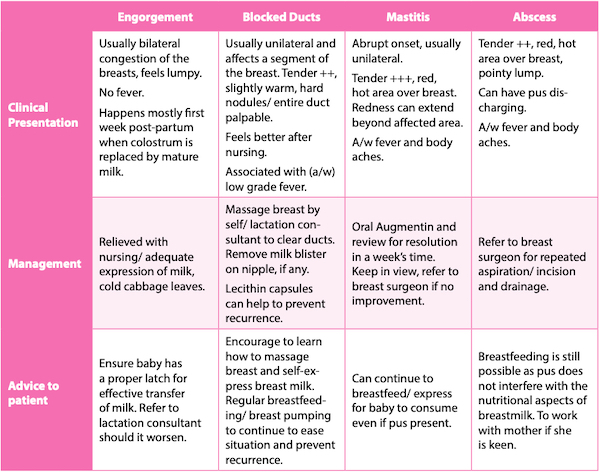
- Common breast issues and management – refer to Table 1.
During the webinar, we received a large number of wide-ranging questions on postnatal blues and depression that we could not fully address. Hence, I would like to share more on the challenging postnatal period that many mothers experience and allow us to better manage them in time to come.
Postnatal blues and postnatal depression
Postnatal blues are generally benign and self-limiting, with a prevalence that ranges from 30% to 75%.1 Symptoms typically start within the first couple of days after delivery, peak around one week, and taper off by the end of the second week post-partum. Symptoms include mood lability, irritability, tearfulness, generalised anxiety, and sleep and appetite disturbance. It arises due to a combination of major hormonal change, stress, sleep deprivation and fatigue. It is, however, important to note that up to 20% of women with blues will go on to develop major depression in the first post-partum year,1 hence it is important that we actively keep a look out for our new mothers.
Postnatal depression (PND) is a lot more sinister and if left untreated, has long-term adverse impacts on both the mother and child. For the mother, the episode can be the precursor of chronic or recurrent depression. For her child, a mother's ongoing depression can contribute to emotional, behavioural, cognitive and interpersonal problems in later life.1 To make matters worse, a woman's risk of recurring PND with subsequent children is estimated at 50% to 100%.
Behind the stigma
A local prospective study showed that the prevalence of PND in Singapore, when considering both major and minor depression, was 6.8%.2
However, this number might be under-reported due to the stigmatisation involved with PND. It is estimated that at least 50% of PND cases go unrecognised.3 The image of an "unhappy mother" is highly undesirable as having a baby is supposed to be a happy event. Hence, new mothers often hide their distress. In addition, mothers are reluctant to label their babies as the cause of their mood disorder.4 Isolation, especially with a nuclear family set-up in our modern society, makes it difficult for mothers to seek help. Furthermore, anxiety may be the predominant symptom in PND, which can be mistaken as common anxiety from the new mother by healthcare providers.5
Symptoms of PND closely mirror those of clinical depression, with women experiencing intense feelings of sadness, anxiety, despair and irritability that interfere with daily function. It often presents one to three weeks after childbirth and can occur for up to one year.
Well-researched risk factors for PND include any prior history of depression, inadequate social support, poor quality of the mother's relationship with her partner, and the presence of life and/or childcare stress.1
Pain and physical difficulty breastfeeding are also shown to increase the risk of PND.6 Mothers often report that they believed that breastfeeding would be straightforward. When they encountered difficulties, they felt guilty, let down and upset by the experience, believing that they have "failed". This further enhances their feelings of inadequacy and adds on to their despair. It has been shown that women with negative early breastfeeding experiences were more likely to have depressive symptoms at two months post-partum. Therefore, women with breastfeeding difficulties should be screened for depressive symptoms7 in early stages to detect PND. It is also important for us to pick up women with breastfeeding challenges and provide them with timely support to prevent the escalation of the situation, thereby reducing risk of PND.
Identification and treatment
The majority of PND cases are identified by primary care (41.3%), followed by obstetricians (30.7%), then mental health providers (13.0%).4 Identifying mothers with high risk factors and who are not coping well is essential to reduce the risk of postnatal blues transiting to PND. Early identification of high-risk cases, even at the time of pregnancy, can prove to reduce the incidence and severity of PND (eg, by providing psychiatric support to mothers who have known history of depression during pregnancy and after delivery). The Edinburgh Postpartum Depression Scale (EPDS) is currently the recommended screening tool for PND.
Social support is deemed as an important protective factor for PND.1 Sources of support can come from their spouse, relatives, friends or even healthcare professionals. There are also different types of social support; eg, informational support (where advice and guidance are given), instrumental support (practical help in terms of material aid or assistance with tasks) and emotional support (expressions of caring and esteem). Healthcare providers are often referred to for up-to-date and accurate informational support. Hence, it is important for us to familiarise ourselves with knowledge to care for new mothers or, minimally, be aware of resources we can refer new parents to.
The majority of PND cases can be treated outpatient. Patients who have severe depression, especially with the intent of harming self and baby should be hospitalised. For mild to moderate depression, psychotherapy has proven to be an effective modality. Pharmacotherapy is added for those with severe PND.4 Breastfeeding mothers are often concerned about the use of drugs and its transfer to the baby. Hence, it is prudent for us to understand the needs of the new mother prior to commencement of treatment, thereby improving compliance.
In summary, PND is more common than we thought. Identifying high-risk cases early and providing timely intervention will help to reduce the long-term effects of PND on both mother and child. Supporting mothers to have successful initiation and maintenance of breastfeeding for at least three months has also been shown to lower the scores on the EPDS.8