The majority of specialists had issues with the implementation of Integrated Shield Plan (IP) panels, and the implementation of IP panels and pre-authorisation had an impact on patients' quality of care.
Many Singaporeans depend on IPs to cover for their hospitalisation costs in private hospitals. The IPs cover the costs of the hospital facilities, room and board, as well as the fees of the private specialists. Private specialists, especially those who treat mainly Singaporeans with IP policies, are particularly affected when there are changes in these policies.
In 2016, the Health Insurance Task Force (HITF) came up with several recommendations to tackle the rising cost of health insurance in Singapore, including the introduction of fee benchmarks, implementation of panels of preferred healthcare providers, and pre-approval of medical treatments.1 Accordingly, the Ministry of Health (MOH) came up with fee benchmarks for over 200 common surgical procedures.2 IP providers implemented panels of preferred specialists, who provide inpatient treatment at rates that have been pre-determined by the IP providers. Patients are incentivised by their IPs to get treated by panel specialists, as they incur lower upfront costs and benefit from a longer period of post-hospitalisation cover. Subsequently, IP providers implemented a pre-authorisation process in which specialists are required to submit information on patients' medical conditions, proposed treatment and estimated costs for IP provider's approval before hospitalisation.
Anecdotally, many specialists had expressed their concerns about the implementation of the panels as well as the pre-authorisation process. These complaints included:
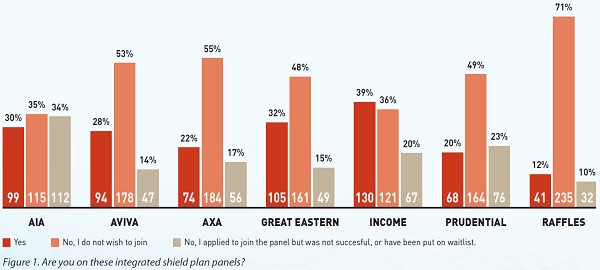
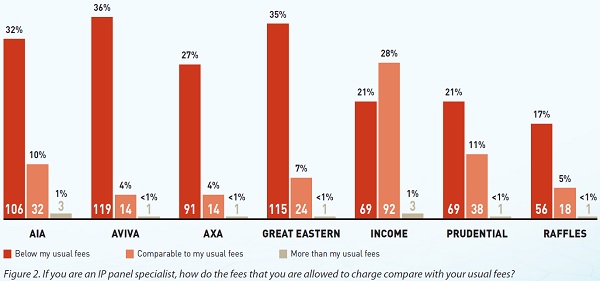
- Panel specialists are remunerated insufficiently, often below the lower range of the fee benchmarks;
- It is difficult for doctors to get on some panels;
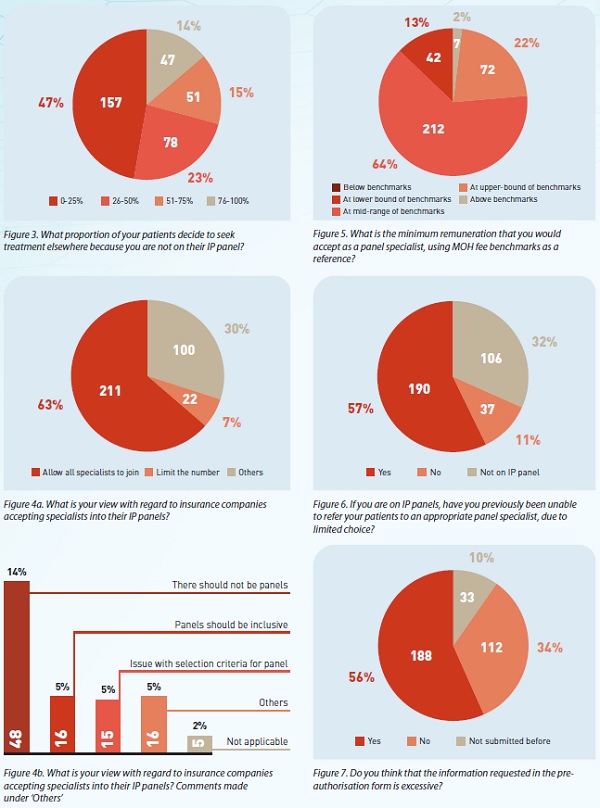
- It is difficult for panel doctors to refer patients to an appropriate specialist due to limited choices;
- The amount of information requested in the pre-authorisation form is excessive;
- The pre-authorisation process causes undue delay in patients' treatment; and
-
The amount pre-authorised is insufficient to cover the total bill.
SMA thus commissioned an online survey to obtain specialists' opinions on these issues.
The survey was conducted on the online SurveyMonkey platform, between 18 September and 2 October 2020. An invitation to participate in the survey was emailed to all SMA Members on the mailing list on 18 September 2020, and a second reminder was sent on 27 September 2020. In addition, a direct link to the survey was provided to SMA Council members for the purpose of distribution via WhatsApp chat groups. The survey comprised 25 questions (https://bit.ly/2R6OwPp). Specialists were required to provide their names and MCR numbers, as a measure to improve the validity of the survey.
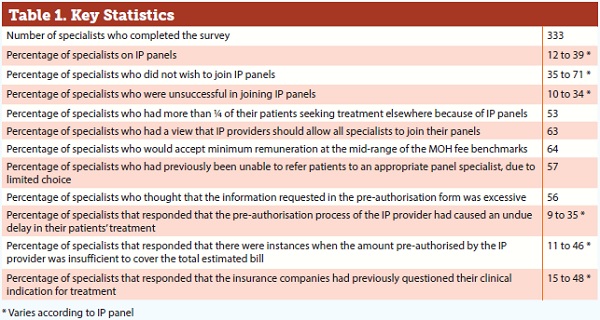
There were 333 specialists who completed the survey, of which 97% were practising in private practice and 3% in restructured hospitals. The summary and discussion of the results of the survey are as follows:
Conclusion
As far as we know, this is the first comprehensive survey of specialists’ opinion on IP providers. The number of specialists who participated in this survey is around 22% of the approximated 1,500 specialists in private practice in Singapore. The number of specialists could have been limited by the requirement for specialists to provide their names and MCR numbers. The results could be viewed as a reflection of the opinions of the general body of specialists. However, there could be selection bias, in that those with issues with the IP providers could have chosen to participate, while those who had no issues did not. In addition, as this was an electronic survey, specialists who did not have email or WhatsApp chat group access would not have been able to participate.
In summary, this survey shows that the majority of specialists surveyed had issues with IP panels, in terms of remuneration, difficulties in getting on the panels and patients having to seek care elsewhere. Patient referrals were also compromised due to limited choice of panel specialists. The pre-authorisation process sometimes caused delays in patients’ treatment and there were instances when the pre-authorised amounts were insufficient to cover the total bill. During the pre-authorisation process, specialists were often asked to provide excessive information, and IP providers frequently questioned specialists’ indications for treatment.
We hope this survey will assist IP providers, MOH and the respective professional bodies in their efforts to improve IP policies, for the benefit of all parties concerned