Point-of-care ultrasound (POCUS) has enjoyed increased interest and exposure over the last decade. A quick, non-invasive investigation modality is always a welcome tool in a clinic. Also, because ultrasound allows one to actually see in real time what we can only infer through history, palpation and/or auscultation, it is an exceptional feedback tool of the clinical examination.
POCUS was endorsed by the American Medical Association in 2001. Doctors from diverse specialties can, should, and have been trained to use ultrasound within their scope of practice.
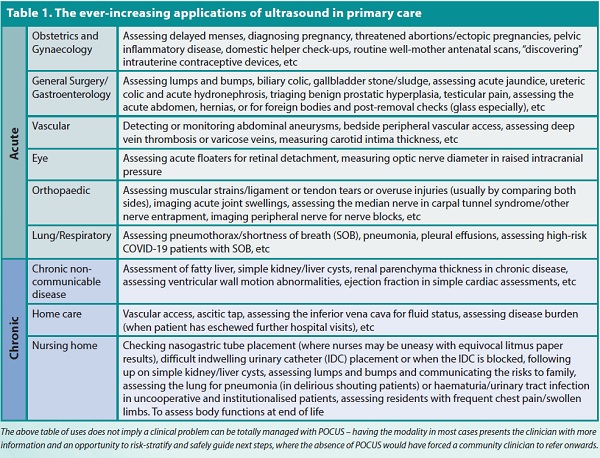
How ultrasound is being used
Traditional piezoelectric probes have varying frequency ranges allowing proper penetration, image acquisition and good resolution of different organs. Very commonly, primary care doctors started off using POCUS within the familiar realms of obstetrics (acquiring the basic parameters for antenatal care – fetal presentation(s), amniotic fluid index, cardiac activity, placentation and estimated fetal weight). As practice grew, physicians have found many other uses for it. With the advent of multi-frequency probes via microchip technology (eg, the Butterfly iQ), the opportunities have only multiplied (see Table 1).
One simply starts by scanning themselves first. It was interesting to discover renal cysts and a gallbladder polyp in my scans. It was instructional to discover my biceps tendon had been transposed anteriorly by the surgeon during the operation for a bad shoulder injury almost a decade ago. I had to correlate it with the operation notes on the National Electronic Health Record (accessed via another kind colleague's account! Ahem!).
I am blessed to have been exposed to routine bedside ultrasound work in my postings in general surgery and urology during my medical officer days. This foundation made getting started much easier. Getting a certificate in General Abdominal Ultrasound at the Singapore General Hospital's Postgraduate Medical Institute certainly helped to allay some fears. But this was not enough though.
Pitfalls of POCUS
The problem with early adopters is that the naysayers are mostly right.
A POCUS practitioner does have to heed the concerns of their vastly more experienced radiology colleagues, because ultrasonography is operator-dependent. You will not see pathology if you are not even aware of its existence or what it is supposed to look like. Continuous learning is thus essential. Certain organs are much harder to learn to scan (eg, cardiac) than others. Having said that, the chances for absolute safe practice in a clinical environment reduces significantly as one moves into the community.
Even with the appropriate certification and background work, I have been caught out before (more than I would have liked, but thankfully less). I am forever indebted to the many colleagues and teachers who have given open, constructive feedback and probed my enthusiasm with sincere questions and pointers. I am also grateful to friendly radiographers who graciously provided image acquisition tips. Consistent, high-quality feedback is essential wherever one is practising.
However, an inquisitive mind grounded in the basic medical sciences and the principles of ultrasound is also required to push the envelope and find new areas of application. Take the role of lung ultrasonography for risk-stratification of COVID-19-positive patients for instance, borne more out of necessity for lack of other imaging resources and a need for reducing patient contact and maintaining sterility.
Self-learning via multiple free and paid online websites, and attending local or overseas courses (out of one's pocket) certainly helped too. Of note, one should try to avoid courses the ultrasound teaching community refer to as “Pump and Dump", where techniques are taught or quickly demonstrated during the session which leaves no avenue for feedback for further practice on image acquisition – the certificate is useless then.
The local scene
Pre-COVID-19, there were fledgling courses organised by the National University of Singapore for POCUS-related work, but the pandemic had since put a stop to that development. It was saddening to hear that courses were suspended after many years of background work to bring accredited teaching to Singapore. I look forward to those courses resuming soon.
But while COVID-19 took away the teaching, it brought patients closer to accepting the bedside scan. Especially since many simply did not want to visit the hospital or anywhere else.
Ultrasound probe companies have not been slacking either. As we may be aware, there are high distribution costs after the Health Sciences Authority's approval for the machine/probes, which may bump the retail price of a portable ultrasound set beyond S$15k when it is being sold for around S$4k to S$5k elsewhere in the world. With more practitioners and growing interest in the devices, it would not be unrealistic to expect better probes at a much cheaper price point in the near future (one can already buy wireless probes for veterinary medicine on AliExpress and Taobao for approximately S$2k). Battery life, heat management, improved portability, cloud storage, remote consulting and artificial intelligence-guided image acquisition and labelling are some of the common trends in this space. Sonosite (Fujifilm), Clarius, EchoNous and GE Healthcare are some ultrasound-probe companies that come to mind.
It is also heartening to learn that medical students are now given the opportunity to use bedside ultrasound in their pre-clinical years (some American universities even presented students with a probe together with their white coat). I wonder if they are allowed to bring the probe to the dissection hall (pre-dissection)? It is hoped that this new group of students will come to find more high-value applications to bedside ultrasound and break the boundaries of clinical medicine for the benefit of all patients.
Non-clinical perks
One of the greatest joys of practising ultrasound personally has to be documenting my third child in utero – from an intrauterine gestational sac, to her break-dancing with her stubby hand and feet at 12 weeks, to thumb-sucking, giving me the middle finger on the scan when she was at 20 weeks and making me guess her gender (I searched high an low for testes of course!).
I am immensely satisfied by my postgraduate journey to learn POCUS, and I look forward to discussing POCUS image with and learning from my colleagues in the near future!
