Population ageing, accompanied by a tandem rise in neurocognitive disorders such as dementia and stroke diseases, as well as adults with intellectual impairment, have fuelled the rise in the number of persons with cognitive impairment (PCIs) today. As cognitive competence is a necessary prerequisite for advance care planning (ACP), PCIs may lack the mental capacity to meaningfully engage in care planning. However, as enunciated in the Mental Capacity Act (MCA), cognitive impair-ment does not per se equate to a lack of mental capacity, and a person is assumed to have mental capacity unless proven otherwise. Mental capacity pertains to the ability to understand, retain and weigh information to enable informed decision-making and ultimately communicate the decision. This article proposes relevant practice points that can facilitate ACP for PCIs.
Optimising conversations
For a start, as neurodegenerative conditions are progressive, ACP should be conducted as early as possible in the illness trajectory when the person first presents with cognitive concerns before mental incapacity sets in. In dementia for example, where the prodromal stage of mild cognitive impairment (MCI) is a recognised clinical entity, the MCI phase would be the ideal time to engage in ACP conversations. Furthermore, conversations and decisions pertaining to care planning should be conducted under optimal conditions as there can be fluctuations in cognitive competence. Delirium is a case in point, and conditions such as Lewy body disease characteristically present with fluctuations in mental state. Hence, it is important to time ACP conversations to coincide with the patient's optimal mental state.
PCIs can be assessed on their (1) ability to appreciate the impact and prognosis of their illness and (2) desire to enter into ACP conversations. There are four possible profiles that can emerge (summarised in Table 1), and the approach to ACP should be tailored to each profile specifically.
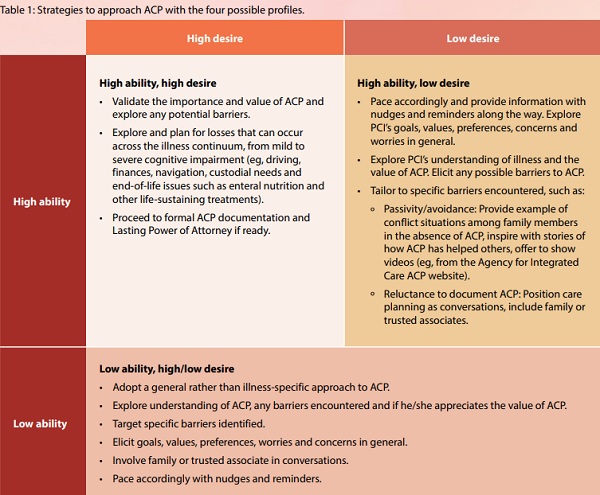
High ability, high desire
This is the ideal scenario where the PCI possesses a good understanding of his/her condition and appreciates the value of ACP. Hence, it might be possible for ACP to be pursued with greater depth to encompass not only issues surrounding end-of-life care, but also a stage-specific plan that explores the deficits experienced at the different stages of the illness. For example, issues pertinent to mild to moderate dementia such as giving up driving, allowing the caregiver to manage medication and finances, and the use of Global Positioning System trackers can be discussed.
High ability, low desire
PCIs may have adequate mental capacity to comprehend the prognostic ramifications of their progressive illness but remain hesitant about ACP. For those who have not given much thought to the matter, information on the importance of ACP can be provided while pacing alongside and accompanying the PCI, and providing him/her with nudges and reminders along the way. If the PCI adopts the acquiescent stance of entrusting future decisions to loved ones, one can provide examples of real-life scenarios where families find themselves in a quandary, having to make difficult decisions on behalf of the person, or when conflicts arise due to differing opinions.
There may also be those who opine that there is no need to make formal care plans as they have casually shared their preferences with those they trust, or may express reservations about the need for formal ACP. Positioning care planning as conversations would be appropriate in such instances, as is the involvement of family members or trusted relatives and friends. The emphasis should be on understanding the PCI's goals, values, priorities and concerns. By building rapport and trust, one can attempt to draw out the PCI's desires and fears, while concurrently seeking out what is important to him/her with the aim of helping him/her live well in the present while also thinking about and planning for the future.
Low ability, high or low desire
Persons under this category are usually more advanced in their cognitive deficits and are characterised by their lack of mental capacity to engage in meaningful discussions. Although intellect and mental capability are compromised, PCIs may still retain the ability to share their personal perspectives, which are often founded more on subjective feelings, long-standing values and preferences. As such, adopting a general approach to care planning might still be possible if they are assisted in the process. Through the personal narratives expressed by the PCI, one can better appreciate his/her life goals, concerns and what matters to him/her, thereby assisting the PCI to navigate care planning. With his/her consent, it would be appropriate to involve surrogate decision-makers during ACP conversations so that they can be privy to the PCI's thoughts and preferences. Having these conversations over time would help to engender trust and familiarity, and ultimately allow care professionals and surrogates to make shared decisions in the best interest of the PCI.
Facilitating ACP
As cognitive deficits may render it challenging for PCIs to articulate their thoughts, assisting them with prompting and paraphrasing can help. Communication strategies such as motivational interviewing and negotiation can also be employed to facilitate conversations. It is important to be intentional in engaging PCIs and to find means to communicate in a manner that works for them. This can include using visual aids and speaking in familiar languages to assist them in their understanding and expression. Deficits in short-term memory may constrain the ability of PCIs to hold information in their minds long enough to allow adequate processing and decision-making. Hence, assisting with "memory prostheses" by way of repetitions and re-presentations of the same information can be utilised as means of bolstering PCIs' mental capacity, to enable them to make and express a choice. If the person is able to consistently make the same choices with these aids, it may be construed that the choices are indeed what the person desires. These practices are aligned with the MCA wherein medical professionals are called upon to undertake practicable steps to help the PCI make informed decisions.
Today, there is growing consensus that ACP should be process-oriented rather than a one-off transaction in completing checkboxes and forms. Research has shown evidence of increased rates of ACP completion through efforts at continued education and conversations over time.1 Direct and regular one-to-one engagement promotes receptiveness while fostering rapport and trust in pacing alongside the PCI. As ACP is a multi-stage process, patience is crucial and one should move to the next stage only when the PCI is ready.
As a key objective of ACP is to prepare individuals for the end of life, it is even more critical that practitioners are sensitive and mindful in the conduct of ACP. It has been found that PCIs often lack an adequate understanding of dementia and its prognosis.2 Furthermore, there may be communication gaps between patients and their physicians, and between patients and their family members. Therefore, ACP conversations can help to clarify and deepen patients' understanding, and allow them the opportunity to share their values, priorities and concerns with both their physicians and families. In particular, in pacing with patients and revisiting discussions as the disease progresses, the process of ACP may allow patients to become more prepared to discuss their end-of-life care preferences over time.
In an oriental setting like Singapore, having time to prepare and engage families is especially important. Family members generally play a pivotal role in ACP discussions, given the culture of familial and collective decisionmaking. The presence of trusted family members during ACP conversations will enable them to hear and appreciate what matters to the PCI, which would in turn incline them to honour his/her preferences and make decisions in his/her best interest when the PCI loses mental capacity in the future, notwithstanding changing circumstances.
Finally, even as we involve families, surrogate decision-makers and care professionals to assist the PCI in decisionmaking, the ethical imperative demands that we elicit what matters to him/her, uphold the primacy of his/her wishes and make every effort to respect him/her. We would do well to avoid being paternalistic in imposing our opinions and wishes on the PCI who is ultimately vulnerable.
