Singapore is at the forefront of a demographic transformation. With one in four citizens projected to be over the age of 65 years by 2030, the need to proactively address ageing and its associated burdens on the healthcare system is more urgent than ever. As a society, the transition from reactive disease management to proactive healthspan extension is needed. This is where the discipline of precision geromedicine (colloquially known as healthy longevity medicine) becomes essential.
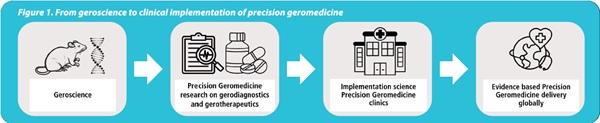
Precision geromedicine is an emerging evidence-based medical discipline rooted in geroscience. It is grounded in the understanding of the biological mechanisms of ageing and applies these insights in clinical practice. By integrating gerodiagnostics (using biomarkers of ageing) and geroprotective interventions, precision geromedicine shifts the paradigm from treating age-related diseases to targeting ageing itself.1
Why precision geromedicine, and why now?
Our current healthcare models are not equipped to handle the impending surge in multimorbidity and syndromes such as frailty. In a 2024 position paper published in Geroscience, we outlined how geroscience is being translated into actionable clinical practice via the framework of healthy longevity medicine.2 This new medical discipline aims to optimise health and extend healthspan by targeting ageing processes across the lifespan.3 The target population includes adults with and without chronic diseases, and excludes individuals who are terminally ill or have severe cognitive impairment.
Singapore's context is uniquely well suited for adopting and leading in this field. With its robust healthcare infrastructure, forward-thinking policy support and ageing population, the city-state presents an exceptional opportunity to demonstrate the value of precision geromedicine in improving population health outcomes.
Key concepts and tools
There are several concepts that underpin precision geromedicine.
Geroscience
The core of geroscience is the hypothesis that ageing is the major risk factor for chronic diseases such as cardiovascular disease, diabetes and neurodegeneration. Targeting the biological hallmarks of ageing, such as cellular senescence, genomic instability and loss of proteostasis, can delay or prevent these conditions.4
Gerodiagnostics using biomarkers of ageing
Unlike chronological age, biological age provides a dynamic, individualised measure of physiological decline. Biomarkers of ageing, ranging from biological to clinical and digital markers, are now partially validated for clinical use. These biomarkers are defined as quantitative parameters of an organism that, alone or in combination, predict biological age and ideally reflect its change in response to interventions.5 The field is advancing in how these markers can be integrated into routine care for risk stratification and to guide gerointerventions.6
Gerotherapeutics
A gerotherapeutic is any non-pharmacological or pharmacological intervention that targets the biological processes of ageing, aiming to prevent, delay or treat multiple age-related diseases simultaneously. Examples of gerotherapeutics include:
Digital monitoring
Continuous monitoring is used to track real-time changes in an individual's behaviours, physiology and health status, incorporating predictive analytics and machine learning.9 These tools can detect subtle deviations from a person's baseline, enabling early and precise interventions.
The concept of digital twins – virtual replicas of individuals built from integrated health data – is also under exploration. These could eventually allow clinicians to simulate and optimise interventions before applying them in real life.
Building the infrastructure
The NUS Academy for Healthy Longevity and the Healthy Longevity Medicine Society (HLMS) are leading efforts to institutionalise precision geromedicine as a distinct medical discipline. The Academy focuses on human research in gerodiagnostics and gerotherapeutics and provides postgraduate training across all sectors engaged in the healthy longevity space, including accredited professional medical courses in healthy longevity. The Academy is also currently developing a Master in Healthy Longevity programme. Early cohorts have already shown the value of our education in upskilling clinicians to adopt a proactive, systems-level approach to ageing. HLMS in turn serves as the international professional body defining clinical guidelines, fostering interdisciplinary collaboration and supporting ongoing research in precision geromedicine.
Challenges and opportunities
We recognise the challenges in establishing a new medical discipline. Regulatory pathways for gerodiagnostics and gerotherapeutics are still in their infancy. Longitudinal data on the safety and efficacy of gerotherapeutics is still being gathered.
The Department of Health in Abu Dhabi, UAE was the first governmental body to set standards for healthy longevity medicine centres. This framework, established in collaboration with HLMS and the Institute for Healthier Living Abu Dhabi, marks the first formal recognition of the field and sets a precedent for other nations. Singapore is well positioned to lead global efforts in validating ageing biomarkers, demonstrating the population-level benefits of gerotherapeutic interventions and, ultimately, standardising care.
We invite interested healthcare practitioners to engage with the NUS Academy for Healthy Longevity to co-create the future of optimised health for ageing individuals. Precision geromedicine is not merely about living longer; it is about living better, with purpose, resilience and independence.
