Introduction
Patient-centred care is care that is "respectful of and responsive to individual patient preferences, needs and values, and ensuring that patient values guide all clinical decisions."1 It has been associated with better adherence and quality of care, as well as improved health outcomes for long- term conditions (LTCs), leading to lower healthcare utilisation and cost.2,3 The ideals of patient-centred care require the holistic healthcare professional (HCP) to skirt at least two complex tasks within the confines of a consultation: (1) understanding patients as holistic persons with preferred values and goals and (2) providing medical expertise that will improve the patients' clinical outcomes. Both are necessary to improve a patient's long-term health.
Is our current ambulatory model of care able to achieve this? The short answer is: not always. Most healthcare systems around the world have to deal with patients with acute episodic conditions, which usually respond predictably to the prescribed treatment (often medication or a surgical procedure) and go away once the treatment is completed. The typical consultation, where an HCP might address a presenting complaint, perform a focused clinical examination and prescribe appropriate therapies based on evidence-based guidelines, may be extremely effective for the management of acute illnesses. By building on this model, Singapore's healthcare system has become one of the most efficient in the world. However, the typical model may not work so well for people living with LTCs.
The unique challenges of LTCs
Unlike acute illnesses, LTCs such as diabetes, hypertension and hyperlipidaemia, once established, stay with a patient for the rest of their lives. As they live their lives, our patients make decisions and choices every day that impact these LTCs. These include choosing what food to eat, whether to take the bus or a cab, or whether they take their medication. In turn, these choices are affected by other factors in their lives, such as the stressors they face, personal preferences, jobs, friends and family members.
Patients see their HCPs for an average of three hours per year (and that's being generous).4 LTCs wax and wane as their lives wax and wane. Sometimes, the LTCs impact their lives; at other times, their lives impact their LTCs. Seldom do these cycles follow the regular scheduled visits through which we provide care. This means that at most times, we are not there when a patient really needs us. This makes it particularly important to build partnerships with our patients to develop a care plan that enables them to make decisions about goals, therapeutic options and self-care behaviours for reasons that matter to themselves. Patients are then more likely to assume responsibility for these care plans and live more effectively with their LTCs.5
Besides the limited time that we have with patients, the relentless drive for efficiency and measurable outcomes may also work against us. We have all been in a situation where patients are queueing outside our door, complaining about the waiting time, while we are trying to get our clinics finished so that we can take a short break for a meal before we begin again. We just want to assess the situation, identify the right treatment, prescribe it and move on. We simply do not have time to think about why a patient does not want to take particular medications or is not able to engage in regular physical activity. Nor are we able to have discussions about more general issues in their lives that, although not appearing to be directly related to their LTCs, might be the only stumbling block to living well with the condition.
As a consequence, the prescribed goals may not align with the patient's own goals and they may not follow through with the plans. If the prescribed goals are not met, patients may (rightly or not) perceive themselves as being judged by their HCPs, particularly with the emergence of terms such as "non-compliance", "non- adherence", or even "lazy" and "naughty" used to describe our patients (we've all said this, so there's no point denying it). In the wake of patients perceiving themselves as a "failure", frustration and resignation may follow, which results in a vicious cycle that ultimately leads to poor outcomes for both the patients and the healthcare system.6
We know that this is happening in our healthcare system. As part of a design thinking work stream under the War on Diabetes, our Ministry of Health (MOH) conducted a number of in-depth discussions with patients living with diabetes who received care across a broad spectrum of care contexts. When asked about their experience with diabetes care, some patients brought up what they perceived to be the judgemental, unfeeling attitude of some HCPs:
"This guy, he whack me, you know – the way he talk. I just sit there and let you whack. You are right lah, I am wrong. Talk to you no point, I just get my medication [and] go off. He ridiculed me."
"The nurse is very scary also... she told me am I cheating my readings, am I like faking it. she said for this type of reading, you should have some symptoms. which I don't have. And then it's like you don't believe me. What's the point I show you?"
Asked to describe their ideal care experience, the patients mentioned aspects such as being heard and respected by their care team; having goals that were realistic and important to them; and having specific assistance when they had difficulty adjusting their diet and exercise, or managing their complications and treatment side effects.
A Citizen's Jury, comprising 76 members of the public, was subsequently convened by the MOH, in collaboration with the Institute of Policy Studies in 2018. It identified priority areas for improving diabetes care, including the empowerment of patients and caregivers in order to make better care decisions; closing the gap between patients' and HCPs' goals; and enhancing the manner of communication by HCPs, as exemplified by the principles of motivational interviewing, in order to better facilitate the attainment of patients' needs and goals.7 In other words, they wanted care to be more patient-centred.
These concepts are not new. As clinicians, we are taught about effective communication in medical school, and many of us have long recognised the importance of patient engagement. The MOH also urges Singaporeans to take individual responsibility for our own health. Our Minister for Health recognised that healthcare is a partnership between providers and patients when he said, "When we replace 'I' with 'We' and we do it together, 'Illness' can become ‘Wellness.'"8
This is not something that can be applied only to a few "difficult" patients. Previous studies have emphasised that care planning conversations need to be incorporated into routine clinical care rather than part of a side programme.9 As providers, the challenge we face is how we could achieve this while meeting the demands for efficiency and sustainability placed on our healthcare system by an ageing population that suffers from an increasing burden of chronic, non- communicable disease.
Year of Care model of patient-centred care
The Year of Care (YoC) patient-centred care programme was initiated in England in 2007. Modelled partly after Wagner's Chronic Care Model,10 the YoC programme envisaged care delivery in a healthcare system organised to enable partnership between "engaged"or "activated"patients and their HCPs. The ultimate goal is to facilitate patient self-management.
The "House of Care" figure depicts this model. Central to the YoC model of care is the collaborative Care and Support Planning (CSP) conversation. It is the platform on which an engaged patient (left wall) discusses what matters to the patient with the HCP (right wall). In collaborative CSP conversations, both patients and the CSP-trained HCPs work collaboratively to identify areas of need, set goals and decide on specific actionable plans that the patient agrees to undertake to achieve these goals. Barriers to achieving the goals and contingencies, should these arise, are discussed. Commissioning by the healthcare cluster (information technology support, training and health service delivery) forms the base of the house, and organisational processes (electronic medical records, results letter sending and so on) form the roof. Using this framework, YoC UK has been able to improve patients' self-care behaviour and experience of care, as well as enhance teamwork, productivity and job satisfaction among HCPs.11
We discuss some of these aspects in further detail in the following description of a pilot programme that we have undertaken in Singapore.
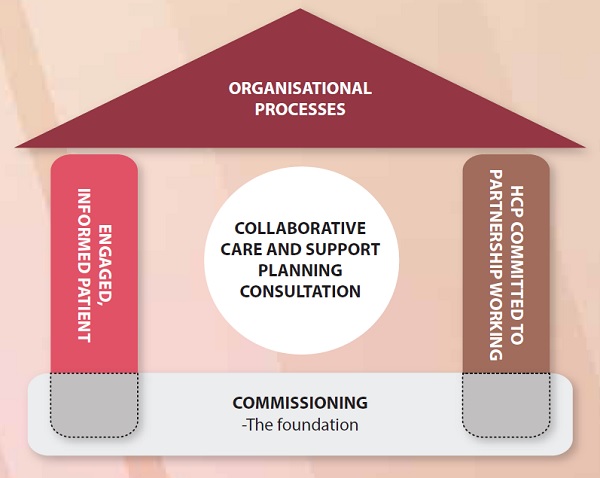
Figure 1. House of Care Framework of the YoC model Reproduced with permission from Year of Care Partnerships
Bringing the YoC model to Singapore
Learning from the YoC UK team
While on attachment to Ninewells Hospital in Dundee, Scotland, from August 2014 to July 2015 on an Academic Medicine Development Award (AMDA) scholarship, Dr Yew Tong Wei experienced first-hand how Scotland adopted the YoC model of care. He was involved in the organisational changes required to enable the model and learnt how to conduct CSP conversations. In doing so, he experienced both the effort involved and the overwhelming benefits of CSP conversations on enabling patient self-care for LTCs. On his return, he found like-minded colleagues at the Division of Endocrinology, National University Hospital (NUH), who realised that this way of delivering care may provide an opportunity to bring patient-centred care to the healthcare system and address some of the implementation challenges we have described. With support from the National University Health System and the Kewalram Chanrai-Enpee Group Research Fund in Diabetes, the team embarked on a plan to implement a YoC-like programme in Singapore, starting with the NUH diabetes clinic.
In July 2017, YoC trainers Drs Lindsay Oliver, Nick Lewis-Barned and Yvonne Doherty travelled to Singapore to train 30 endocrinologists, GPs, nurses, pharmacists and dietitians in facilitating CSP conversations. They focused on several key principles, including approaching patient care as a collaboration between two experts - the patient as an expert in their own lives and the HCP as an expert in treating disease. The trainers shared techniques for uncovering patients' true motivations and goals, as well as tools for working together with patients to develop a plan of action to support them in their self-management and help them achieve their goals.
Implementation at NUH
Arming our HCPs with skills and knowledge alone was not sufficient. Implementing the CSP conversations in the clinical workflow required a redesign of many aspects of care.
The first, and perhaps greatest, challenge, was to make time for CSP conversations in a schedule that barely allows most HCPs time to breathe, never mind to indulge in long conversations with their patients.
To start with, it was determined that CSP conversations would only be carried out once a year, at the time that the patient undergoes his/her annual diabetes screening tests, thus limiting the impact on the HCP's schedule. In order to allocate time for the CSP conversations (20 minutes vs ten minutes for a usual consultation) in packed clinic schedules, the endocrinology team settled on a strategy to start clinics earlier in the day, for example at 8.40 am instead of 9 am to incorporate one CSP session, or at 8.20 am to incorporate two CSP sessions.
Secondly, the team realised that, in a typical consultation, a disproportionate amount of time may be spent on explaining test results to patients. In addition, when the results are sub- optimal, the patient does not have time to process the information and engage in a productive conversation about the possible reasons behind the results, or to discuss the next steps that could be taken. To address this, an easy-to-understand results letter (see Figure 2) was designed, incorporating input from patients to ensure that it would be easily understood. In the redesigned workflow, patients were asked to come earlier for their annual tests and complications screening, and the results in the form of a completed results letter were sent to them ahead of their appointments. This reduced the need to communicate results during the consultation, creating space for the collaborative conversation to take place.
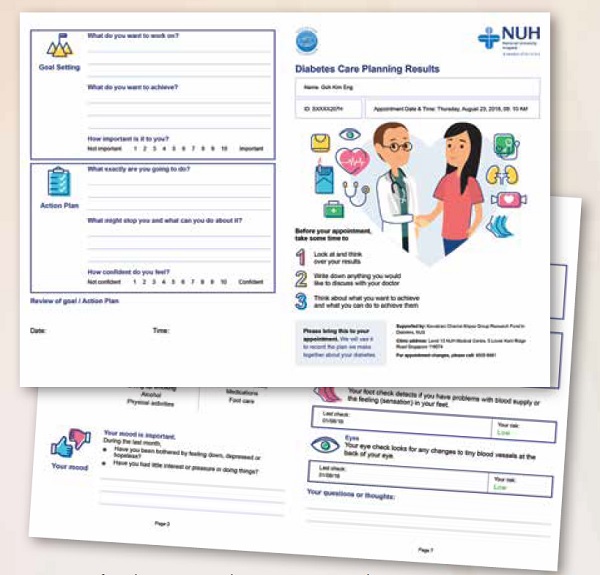
Figure 2. Pages from the NUH YoC Results Letter presenting results, explanations and goal-setting prompts
The prior communication of the results to patients also provided an opportunity for them to better prepare for the CSP conversation. Prompts in the results letter were designed to help prepare patients for the CSP conversation by encouraging them to reflect on their aspirations, needs and concerns prior to the CSP conversation (see Figure 2) and document them, so that the time in the CSP conversation could be more effectively used.
In October 2017, the pilot YoC Singapore programme was launched at the NUH diabetes clinic. Two clinical coordinators were hired for the programme and patients were recruited. In January 2018, the first CSP conversation was held. To date, 176 patients living with diabetes have been enrolled in the programme and 158 have completed at least one CSP conversation. Out of these 158 patients, 59 have completed their first and second CSP conversations. For the most part, both patients and HCPs have responded favourably to the new format.
Implementation challenges
There was a steep initial learning curve for most HCPs. It required them to be skilful in encouraging patients to talk about very personal things, such as their feelings, motivations and fears. This meant adopting a communication style that encouraged patients to surface their goals and concerns and occasionally providing on-the-spot responses to patients' concerns. With practice, the HCPs became more skilful in facilitating CSP conversations.
"It wasn't easy at the start. I found myself reverting to old habits of jumping in and 'lecturing' the patients. This is called the 'righting reflex' - an urge to want to 'make things right' whenever we see a problem," recalled Dr Yew. "It required me to be very mindful, but with practice I can now communicate in a collaborative manner more naturally."
As we have moved into our second CSP visits with our patients, we find that patients also became more effective at articulating their needs and aspirations and working with their HCPs to set goals. Thus, over time, the time required for a CSP becomes shorter, allowing more CSPs to be conducted within the context of our usual practice. This gradual implementation to allow HCPs to adapt is a key part of the process and we would advise any healthcare system considering implementing a similar programme to adopt a staged approach. We are also applying these and other learnings in our patient-centred care study in primary care, called Patient Activation through Community Empowerment/Engagement for Diabetes Management (PACE-D).
We think we can finish here by saying that the challenge of LTCs is far from solved. Implementation needs to be carried out at all levels, including the smallest unit of healthcare delivery - the solo practitioner. But we believe that programmes like YoC offer a glimpse of what is possible, and are a starting point for our journey towards patient- centred care. Whatever we implemented is likely to require future iterations to continuously improve the process, so as to optimise benefits not only in the lives of our patients, but also in the lives of our HCPs. We are delighted to have the opportunity to share some of our early experiences with you as we take this long journey together.
Acknowledgements
The authors would like to acknowledge Dr Khor Ing Wei for her assistance in the writing of this article; the Year of Care Partnerships, National Health Service UK, for training and advice; and the Kewalram Chanrai-Enpee Group Research Fund in Diabetes for funding this programme.